
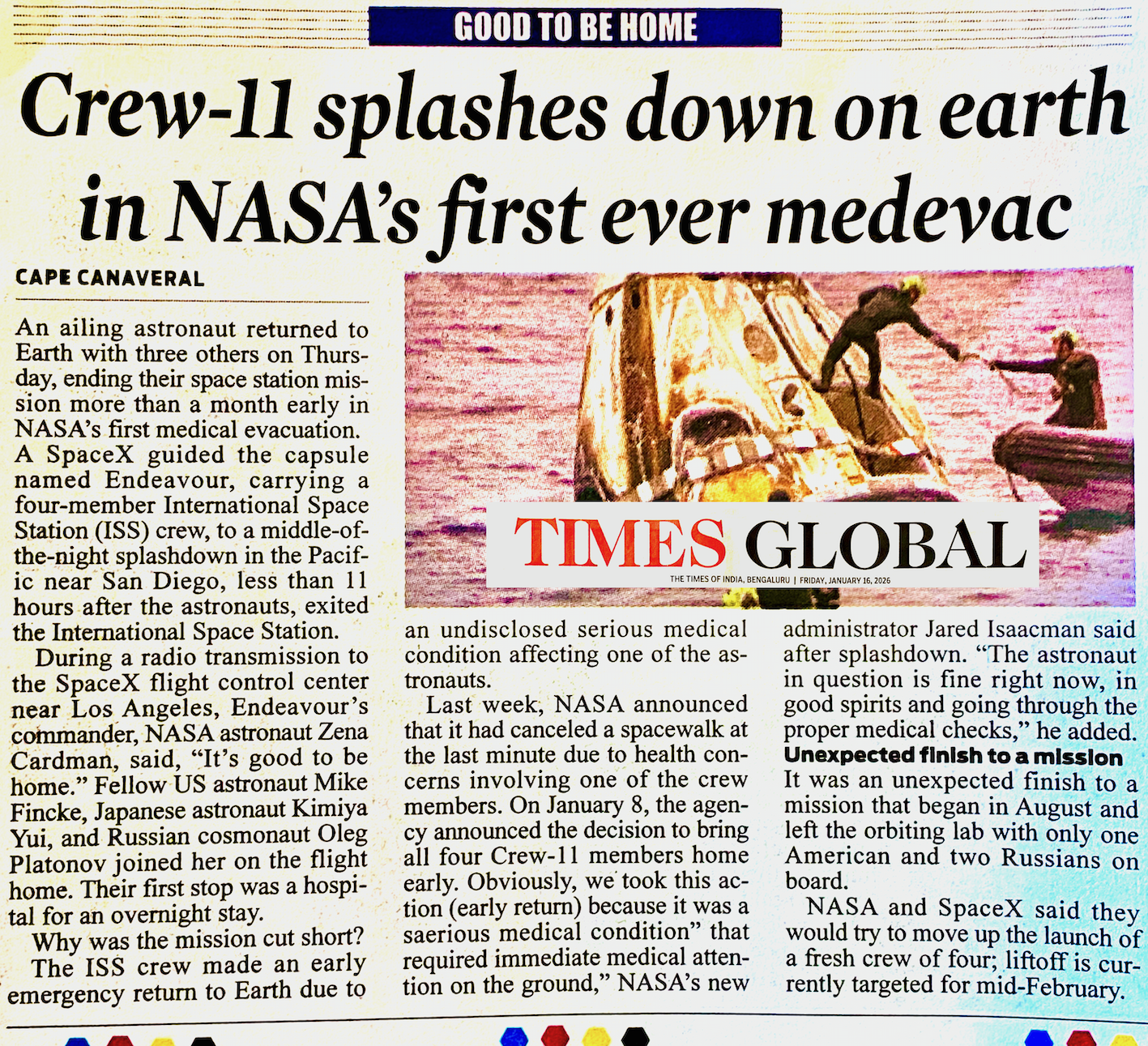
On my way to Patna, I read about Austronotes in The Times of India, which shocked me. One ailing astronaut was brought home less than 11 hours after the astronauts exited the International Space Station and returned to Earth with three others on Thursday, ending their space station mission more than a month early in NASA's first medical evacuation. A SpaceX guided the capsule named Endeavour, carrying a four-member International Space Station (ISS) crew, to a middle-of-the-night splashdown in the Pacific near San Diego.
The astronauts are said to be healthy young adults who must have been investigated, tested, scanned and declared fit to travel. NASA has not shared information about the illness, but I think they were infected by bacteria and fungi left behind by past astronauts who visited the International Space Station (ISS).
In the 1990s, we raised concerns about space travel because bacteria and fungi colonised the space shuttles, and biofilms returned as superbugs. Because the atmosphere around us, the soil, and the water are resistant to antibiotics. These bacteria are likely to become more virulent and be brought back home along with the astronauts. If these bacteria start spreading in the USA, I am sure they will spread faster worldwide. We must begin planning how to manage future epidemics and stop living under the illusion of theoretical idealism.
Scientists have discovered resilient bacteria living in NASA's ultra-clean rooms—organisms capable of surviving the harsh conditions of space! These extremophiles can repair DNA, resist radiation, and could even hitch a ride on future missions to the Moon or Mars. This breakthrough raises both exciting possibilities and serious concerns about planetary contamination. Watch to learn how these tiny survivors could impact space exploration.
WION The World is One News: https://youtu.be/LAdq_ls9UFQ?si=oz8N4Upz-q-G0Ity
A Reflection on Innovation and Leadership at the Indian Institute of Technology Patna
My visit to the Indian Institute of Technology Patna was driven by a simple intention: to share real clinical experience and explore how AI can be applied responsibly in healthcare, with patient safety and human consequence at its core. What I encountered was not opposition, but disengagement—and that is more concerning, because institutions shape not only skills, but values. Healthcare innovation cannot be created through infrastructure, incubation centres, or academic authority alone, especially when detached from clinicians who have carried responsibility for patients, faced uncertainty, and learned from failure.
I visited IIT Patna with a clear purpose to identify collaborators and share lived clinical experience, and explore how AI can share my knowledge, and how AI can be applied responsibly in healthcare, grounded in patient safety, real-world constraints, and ethical decision-making.
AI in healthcare is not merely an engineering challenge; it is a human systems challenge. Bihar has the potential to lead in humane, accessible healthcare. Still, that future will require institutions to move beyond old, doctor-centred hierarchies and model curiosity, humility, and openness to lived experience—because authentic leadership in education is not about titles, but about the example set for students.
When I stepped into a room operating on status logic, GDP logic, and credential logic, while I was speaking from evolution logic, prevention logic, and human-survival logic, those two frames don't resonate. They repel, but the professors did not show up, or were they avoiding contact because my contribution might have threatened their intellectual monopoly?
I felt they are protecting their funding pipelines or systems that reward them, even when those systems are decaying. That's not malice. It's psychological inertia. The fear I sensed when I observed the way they spoke to students. That's how fragile hierarchies defend themselves when they can't compete on originality.
Institutions like IIT Patna do not merely teach technology; they shape mindsets. Students learn as much from what their teachers value as from what they teach. When senior faculty show little curiosity for interdisciplinary dialogue or real-world clinical insight, students quietly learn that innovation is secondary to hierarchy and that listening is optional.
This is not how healthcare innovation is born. Healthcare innovation cannot be created by infrastructure alone, nor by students passing examinations with distinction, nor by incubation centres run in isolation or academic models detached from patient responsibility. Authentic leadership in education is not about authority. It is about setting an example.
Politicians and philontrapists must know you cannot help improve the health of a nation by building hospitals, medical colleges or increasing the number of doctors and nurses. You cannot innovate healthcare without clinicians who have faced uncertainty, failure, and human consequence. AI in healthcare is not an engineering problem alone. It is a human systems problem.
Bihar had the potential to become a national leader in accessible, humane, and scalable healthcare. But that future will not emerge from doctor-centred or institution-centred thinking. It will appear when institutions invite uncomfortable experiences, value wisdom alongside credentials, and model humility, curiosity, and lifelong learning.
I share this reflection not as criticism, but as a call to evolve—for the sake of the students and for the future of healthcare innovation in India.